Infections of the skin and soft tissue
Infections of the skin and soft tissue
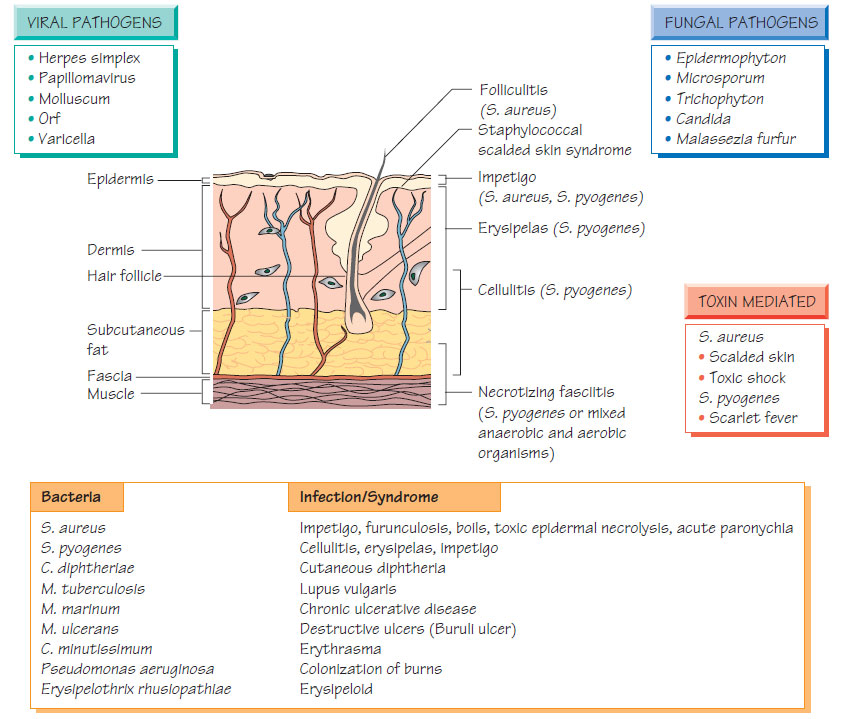
Skin infections spread rapidly by contact, especially in enclosed populations or where sanitation is poor and humidity high. Staphylococcus aureus andStreptococcus pyogenes are the commonest. See Figure for others.
Infections of the skin and soft tissue
Disease patterns
Cellulitis
- Affects all layers of the skin.
- Causes include S. pyogenes, S. aureus, Pasteurella multocida or, rarely, marine vibrios or Gram-negative bacilli.
- Organisms invade via skin abrasions, insect bites or wounds.
- Empirical flucloxacillin should be given until culture results are available. Severe disease should be treated with intravenous antibiotics, including benzylpenicillin and flucloxacillin.
- A rapidly progressive infection that spreads to involve the skin and subcutaneous layers.
- It is caused by mixed aerobic and anaerobic organisms or pure S. pyogenes.
- The condition is characterized by pain, fever and shock, and the infected area may be discoloured.
- Progression is rapid, leading to death in a very short time.
- Surgical resection of infected tissue is critical, supplemented with antibiotics targeted against streptococci, staphylococci, Gramnegative bacilli and obligate anaerobes (e.g. benzylpenicillin, a third-generation cephalosporin and metronidazole).
Erythrasma
This superficial infection of the flexures is caused by Corynebacterium minutissimum - the lesions fluoresce under Wood's light. The organism may be cultured; treatment is with erythromycin or tetracycline.
- A well-demarcated streptococcal infection confined to the dermis.
- The condition is found on the face or shins.
- It is hot and red on examination.
- A modest increase in the peripheral white blood cells and fever occur.
- Treatment is with oral amoxicillin or flucloxacillin given intravenously in severe cases.
Erysipeloid
- Zoonosis found in pig handlers and fisherman caused by Erysipelothrix rhusiopathiae.
- It may be self-limiting but treatment with oral penicillin or tetracycline speeds the response and is needed in rare septicaemic cases.
- Burns are susceptible to bacterial colonization.
- Typical organisms are Pseudomonas aeruginosa, S. aureus, S. pyogenes and, less commonly, coliforms.
- Antibiotic resistance is an increasing problem. Complications include loss of skin grafts and secondary bacteraemia.
Paronychia
This is a common infection in community practice. The cuticle is damaged, which allows invasion with organisms such as S. aureus. There is pain and swelling, followed by a small abscess. The abscess may be drained and antibiotics can be given (e.g. flucloxacillin).
The skin is a large organ that is a window onto systemic infection. Examples of this include:
- the petechial rash of meningococcal septicaemia;
- ecthyma gangrenosum of Pseudomonas septicaemia;
- the splinter haemorrhages of endocarditis;
- skin infarctions due to staphylococcal septicaemia;
- rash as part of a systemic infection (e.g. chickenpox and measles);
- the primary site of herpes simplex infection (see Herpesviruses II);
- the different skin manifestations of toxin-mediated systemic disease: toxic shock syndrome due to Staphylococcus aureus (generalized and palmar rash); scarlet fever due to β-haemolytic streptococci (rash with circumoral pallor, scalded skin and desquamation in neonates).
- Skin infected with human papillomavirus (HPV) shows increased replication, which gives rise to a wart. Papular, macular or mosaic variants occur. Verrucae (plantar warts) are found on the soles of the feet. The virus is transmitted by direct contact, particularly under wet conditions, such as around swimming pools.
- Genital warts (condylomata acuminata) may be transmitted sexually. Diagnosis is usually clinical.
- Virus in condylomata acuminata can be detected by immunofluorescence and nucleic acid amplification test (NAAT).
- HPV is associated with malignancy: cervical (HPV-16 and HPV- 18); and laryngeal (HPV-6 and HPV-11). A vaccine has been introduced that provides sustained immunity against the serotypes associated with cervical cancer.
- Except in immunocompromised patients, warts are self-limiting and resolve spontaneously without scarring. Over-the-counter, topical keratolytic agents (e.g. salicylic acid) are widely used.
- Genital warts may respond to the application of podophyllum by trained staff. Cryotherapy is the second-line therapy
Support our developers




