Tubular Reabsorption
Tubular Reabsorption
Approximately 60% of the filtrate volume
and virtually all of the glucose,
amino acids, vitamins and other valuable
nutrients are reabsorbed in the
proximal convoluted tubule. Much of
this reabsorption is by active transport,
in which cellular energy is used
to transport materials from tubular
fluid to the surrounding capillary network
from which they will reenter the
blood circulation. Electrolytes such as
sodium, potassium, calcium, bicarbonate,
and phosphate are reabsorbed by
ion pumps, which are carrier proteins driven by the hydrolysis of ATP (ion
pumps are described on).
Because an essential function of the
kidney is to regulate the plasma concentrations
of electrolytes, all are individually
reabsorbed by ion pumps specific
for each electrolyte. Some are
strongly reabsorbed and others weakly
reabsorbed, depending on the body’s
need to conserve each mineral. Some
materials are passively reabsorbed.
Negatively charged chloride ions, for
example, passively accompany active
reabsorption of positively charged
sodium ions in the proximal convoluted
tubule. Water, too, is withdrawn
passively from the tubule, as it follows
osmotically the active reabsorption of
solutes.
In the disease diabetes mellitus (“sweet running through”), glucose rises to abnormally high concentrations in the blood plasma (hyperglycemia) because the hormone insulin, which enables body cells to take up glucose, is deficient. As blood glucose rises above a normal level of about 100 mg/100 ml of plasma, the concentration of glucose in the filtrate also rises, and more glucose must be reabsorbed by the proximal tubule. Eventually a point is reached (about 300 mg/ 100 ml of plasma) at which reabsorptive capacity of the tubular cells is saturated. This point is the transport maximum for glucose. Should plasma glucose continue to rise, glucose spills into the urine. In untreated diabetes mellitus the victim’s urine tastes sweet, thirst is unrelenting, and the body wastes away despite a large food intake. In England the disease for centuries was appropriately called the “pissing evil.”
For most substances there is an upper limit to the amount of substance that can be reabsorbed. This upper limit is termed the transport maximum (renal threshold) for that substance. For example, glucose normally is reabsorbed completely by the kidney because the transport maximum for glucose is poised well above the amount of glucose usually present in the plasma filtrate. Should the plasma glucose concentration exceed this threshold level, as in the disease diabetes mellitus, glucose appears in the urine (Figure 32-13).
Unlike glucose, most electrolytes are excreted in the urine in variable amounts. The reabsorption of sodium, the dominant cation in the plasma, illustrates the flexibility of the reabsorption process. The human kidney filters approximately 600 g of sodium every 24 hours. Nearly all of this sodium is reabsorbed, but the exact amount is matched precisely to sodium intake. With a normal sodium intake of 4 g per day, the kidney excretes 4 g and reabsorbs 596 g each day. A person on a low-salt diet of 0.3 g of sodium per day still maintains salt balance because only 0.3 g escapes reabsorption. But with a very high salt intake, much above 20 g per day, the kidney cannot excrete sodium as fast as it enters. The unexcreted sodium chloride holds additional water in the body fluids, and the person begins to gain weight. (The salt intake of the average North American is about 6 to 18 g per day, approximately 20 times more than the body needs, and three times more than is considered acceptable for those predisposed to high blood pressure.)
The human kidney can adapt to excrete large quantities of salt (sodium chloride) under conditions of high salt intake. In societies accustomed to widespread use of foods heavily salted for preservation (for example, salted pork and salt herring) daily intakes may approach or even exceed 100 g. Body weight remains normal under such conditions.However, the acute ingestion of 20 to 40 g/day by volunteers unadapted to such large intakes of salt caused swelling of tissues, increase in body weight, and some increase in blood pressure.
The distal convoluted tubule carries out the final adjustment of filtrate composition. Sodium reabsorbed by the proximal convoluted tubule—some 85% of the total filtered—is obligatory reabsorption; this amount will be reabsorbed independent of sodium intake. In the distal convoluted tubule, however, sodium reabsorption is controlled by aldosterone, a steroid hormone from the adrenal gland . Aldosterone increases active reabsorption of sodium by the distal tubules and thus decreases loss of sodium in the urine. The secretion of aldosterone is regulated mainly by the enzyme renin, produced by the juxtaglomerular apparatus, a complex of cells located in the afferent arteriole at its junction with the glomerulus (Figure 32-10). Renin is released in response to a low blood sodium level or to low blood pressure (which can occur if the blood volume drops too low). Renin then initiates a series of enzymatic events culminating in the production of angiotensin, a blood protein that has several related effects. First, it stimulates the release of aldosterone, which acts in turn to increase sodium reabsorption by the distal tubule. Second, it increases the secretion of antidiuretic hormone (vasopressin, discussed later in the section), which promotes water conservation by the kidney. Third, it increases blood pressure. Finally, it stimulates thirst. These actions of angiotensin tend to reverse the circumstances (low blood sodium and low blood pressure and/or blood volume) that triggered the secretion of renin. Sodium and water are conserved, and blood volume and blood pressure are restored to normal.
The flexibility of distal reabsorption of sodium varies considerably in different animals: it is restricted in humans but very broad in many rodents. These differences have appeared because selective pressures during evolution have resulted in rodents adapted for dry environments. They must conserve water and at the same time excrete considerable sodium. Humans, however, were not designed to accommodate the large salt appetites many have. Our closest relatives, the great apes, are vegetarians with an average salt intake of less than 0.5 g per day.
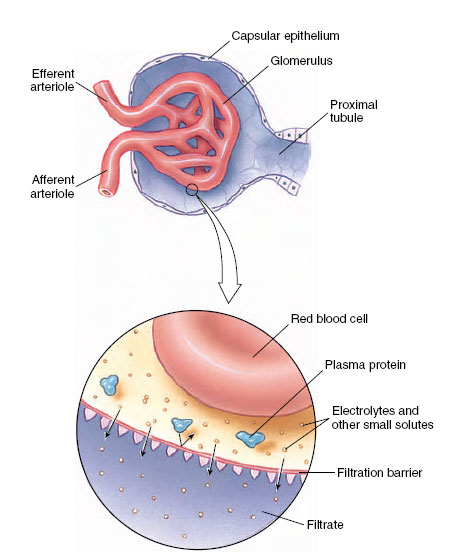 |
| Figure 32-12 Renal corpuscle, showing (enlargement) the filtration of fluid through the glomerular capillary membrane. Water, electrolytes, and other small molecules pass the porous filtration barrier, but the plasma proteins are too large to pass the barrier. The filtrate is thus protein free. |
In the disease diabetes mellitus (“sweet running through”), glucose rises to abnormally high concentrations in the blood plasma (hyperglycemia) because the hormone insulin, which enables body cells to take up glucose, is deficient. As blood glucose rises above a normal level of about 100 mg/100 ml of plasma, the concentration of glucose in the filtrate also rises, and more glucose must be reabsorbed by the proximal tubule. Eventually a point is reached (about 300 mg/ 100 ml of plasma) at which reabsorptive capacity of the tubular cells is saturated. This point is the transport maximum for glucose. Should plasma glucose continue to rise, glucose spills into the urine. In untreated diabetes mellitus the victim’s urine tastes sweet, thirst is unrelenting, and the body wastes away despite a large food intake. In England the disease for centuries was appropriately called the “pissing evil.”
For most substances there is an upper limit to the amount of substance that can be reabsorbed. This upper limit is termed the transport maximum (renal threshold) for that substance. For example, glucose normally is reabsorbed completely by the kidney because the transport maximum for glucose is poised well above the amount of glucose usually present in the plasma filtrate. Should the plasma glucose concentration exceed this threshold level, as in the disease diabetes mellitus, glucose appears in the urine (Figure 32-13).
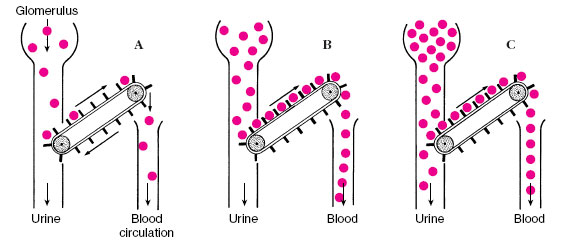 |
| Figure 32-13 The mechanism for the tubular reabsorption of glucose can be likened to a conveyor belt running at constant speed. A, When the concentration of glucose in the filtrate is low, all is reabsorbed. B, When the glucose concentration in the filtrate has reached the transport maximum, all carrier sites for glucose are occupied. If the glucose rises further, C, as in the disease diabetes mellitus, some glucose escapes the carriers and appears in the urine. |
Unlike glucose, most electrolytes are excreted in the urine in variable amounts. The reabsorption of sodium, the dominant cation in the plasma, illustrates the flexibility of the reabsorption process. The human kidney filters approximately 600 g of sodium every 24 hours. Nearly all of this sodium is reabsorbed, but the exact amount is matched precisely to sodium intake. With a normal sodium intake of 4 g per day, the kidney excretes 4 g and reabsorbs 596 g each day. A person on a low-salt diet of 0.3 g of sodium per day still maintains salt balance because only 0.3 g escapes reabsorption. But with a very high salt intake, much above 20 g per day, the kidney cannot excrete sodium as fast as it enters. The unexcreted sodium chloride holds additional water in the body fluids, and the person begins to gain weight. (The salt intake of the average North American is about 6 to 18 g per day, approximately 20 times more than the body needs, and three times more than is considered acceptable for those predisposed to high blood pressure.)
The human kidney can adapt to excrete large quantities of salt (sodium chloride) under conditions of high salt intake. In societies accustomed to widespread use of foods heavily salted for preservation (for example, salted pork and salt herring) daily intakes may approach or even exceed 100 g. Body weight remains normal under such conditions.However, the acute ingestion of 20 to 40 g/day by volunteers unadapted to such large intakes of salt caused swelling of tissues, increase in body weight, and some increase in blood pressure.
The distal convoluted tubule carries out the final adjustment of filtrate composition. Sodium reabsorbed by the proximal convoluted tubule—some 85% of the total filtered—is obligatory reabsorption; this amount will be reabsorbed independent of sodium intake. In the distal convoluted tubule, however, sodium reabsorption is controlled by aldosterone, a steroid hormone from the adrenal gland . Aldosterone increases active reabsorption of sodium by the distal tubules and thus decreases loss of sodium in the urine. The secretion of aldosterone is regulated mainly by the enzyme renin, produced by the juxtaglomerular apparatus, a complex of cells located in the afferent arteriole at its junction with the glomerulus (Figure 32-10). Renin is released in response to a low blood sodium level or to low blood pressure (which can occur if the blood volume drops too low). Renin then initiates a series of enzymatic events culminating in the production of angiotensin, a blood protein that has several related effects. First, it stimulates the release of aldosterone, which acts in turn to increase sodium reabsorption by the distal tubule. Second, it increases the secretion of antidiuretic hormone (vasopressin, discussed later in the section), which promotes water conservation by the kidney. Third, it increases blood pressure. Finally, it stimulates thirst. These actions of angiotensin tend to reverse the circumstances (low blood sodium and low blood pressure and/or blood volume) that triggered the secretion of renin. Sodium and water are conserved, and blood volume and blood pressure are restored to normal.
The flexibility of distal reabsorption of sodium varies considerably in different animals: it is restricted in humans but very broad in many rodents. These differences have appeared because selective pressures during evolution have resulted in rodents adapted for dry environments. They must conserve water and at the same time excrete considerable sodium. Humans, however, were not designed to accommodate the large salt appetites many have. Our closest relatives, the great apes, are vegetarians with an average salt intake of less than 0.5 g per day.
Support our developers




